
Risk Assessment of Dietary Exposure to Organophosphorus Flame Retardants in Children by Using HBM-Data

 , , , , , ,
, , , , , ,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Human Biomonitoring Data
Estimation of the Daily Intake (EDI)
2.2. Dietary Exposure
2.3. Hazard and Risk Characterization
3. Results
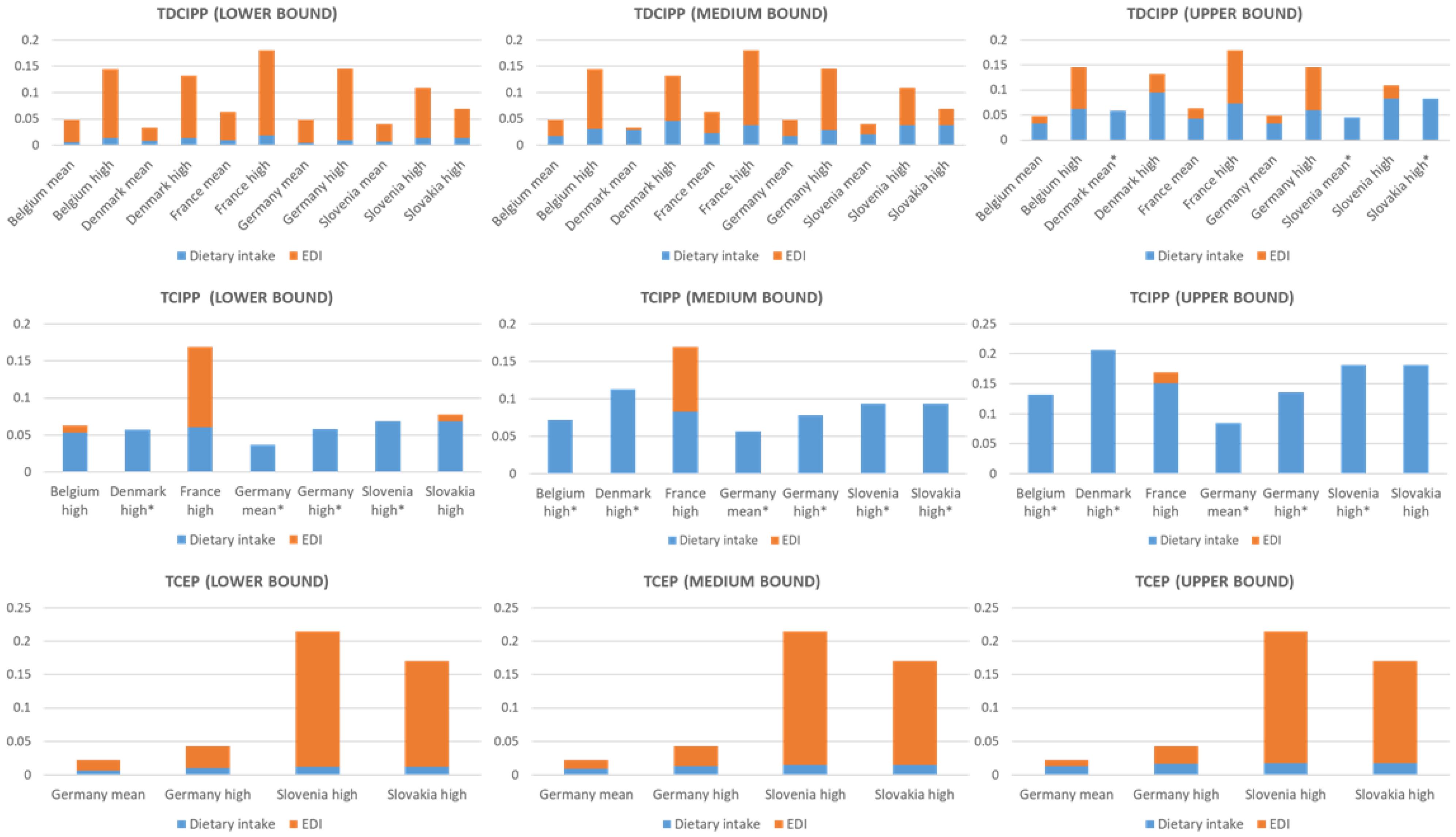
3.1. Estimated Daily Intake (EDI)
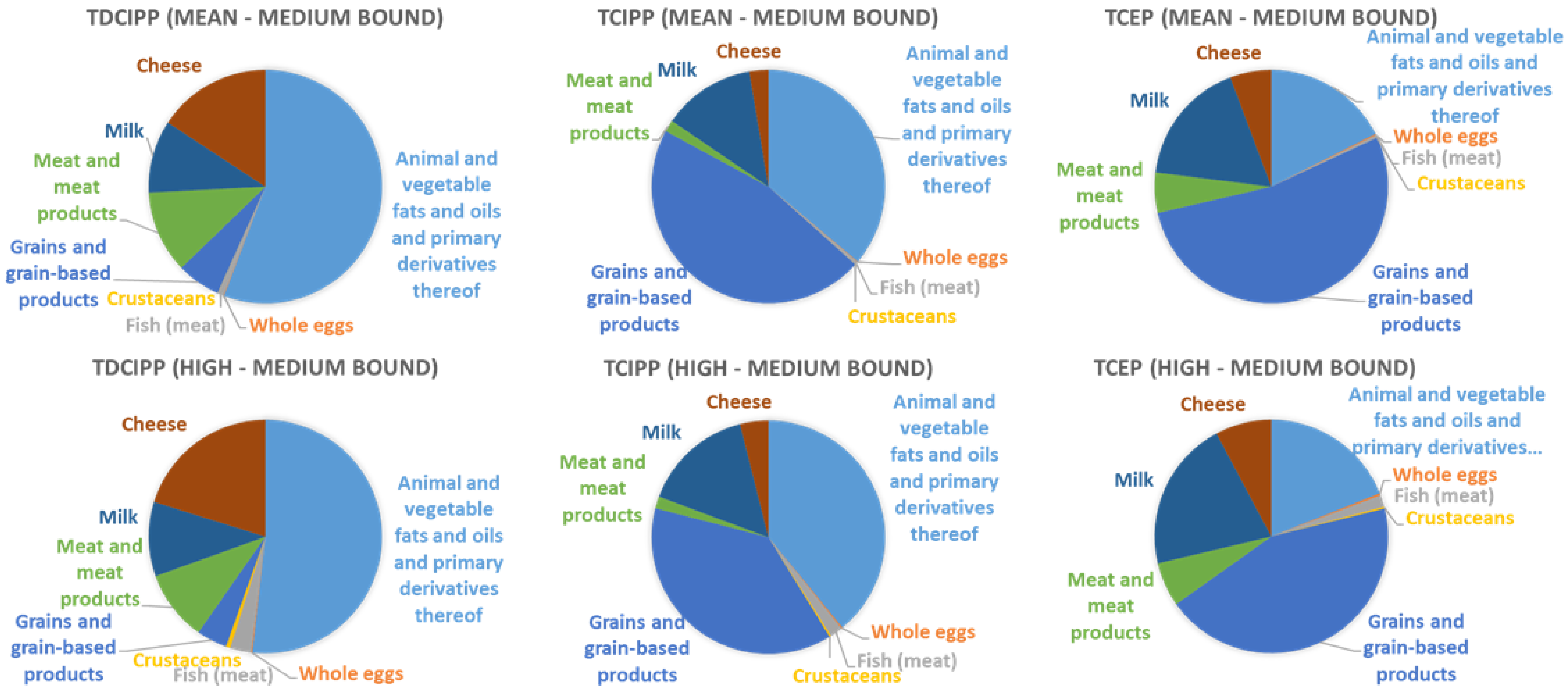
3.2. Dietary Exposure
3.3. Risk Characterization
4. Discussion
4.1. Estimated Daily Intake
4.2. Dietary Intake
4.3. Uncertainties and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hou, R.; Xu, Y.; Wang, Z. Review of OPFRs in animals and humans: Absorption, bioaccumulation, metabolism, and internal exposure research. Chemosphere 2016, 153, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Poma, G.; Glynn, A.; Malarvannan, G.; Covaci, A.; Darnerud, P.O. Dietary intake of phosphorus flame retardants (PFRs) using Swedish food market basket estimations. Food Chem. Toxicol. 2017, 100, 1–7. [Google Scholar] [CrossRef] [PubMed]
- van der Veen, I.; de Boer, J. Phosphorus flame retardants: Properties, production, environmental occurrence, toxicity and analysis. Chemosphere 2012, 88, 1119–1153. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, Q.; Zhong, W.; Yang, L.; Yang, J.; Covaci, A.; Zhu, L. Estimating renal and hepatic clearance rates of organophosphate esters in humans: Impacts of intrinsic metabolism and binding affinity with plasma proteins. Environ. Int. 2020, 134, 105321. [Google Scholar] [CrossRef] [PubMed]
- Blum, A.; Behl, M.; Birnbaum, L.S.; Diamond, M.L.; Phillips, A.; Singla, V.; Sipes, N.S.; Stapleton, H.M.; Venier, M. Organophosphate Ester Flame Retardants: Are They a Regrettable Substitution for Polybrominated Diphenyl Ethers? Environ. Sci. Technol. Lett. 2019, 6, 638–649. [Google Scholar] [CrossRef]
- Li, J.; Zhao, L.; Letcher, R.J.; Zhang, Y.; Jian, K.; Zhang, J.; Su, G. A review on organophosphate Ester (OPE) flame retardants and plasticizers in foodstuffs: Levels, distribution, human dietary exposure, and future directions. Environ. Int. 2019, 127, 35–51. [Google Scholar] [CrossRef]
- Poma, G.; Sales, C.; Bruyland, B.; Christia, C.; Goscinny, S.; Van Loco, J.; Covaci, A. Occurrence of Organophosphorus Flame Retardants and Plasticizers (PFRs) in Belgian Foodstuffs and Estimation of the Dietary Exposure of the Adult Population. Environ. Sci. Technol. 2018, 52, 2331–2338. [Google Scholar] [CrossRef]
- Fromme, H.; Lahrz, T.; Kraft, M.; Fembacher, L.; Mach, C.; Dietrich, S.; Burkardt, R.; Völkel, W.; Göen, T. Organophosphate flame retardants and plasticizers in the air and dust in German daycare centers and human biomonitoring in visiting children (LUPE 3). Environ. Int. 2014, 71, 158–163. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, H.; Zhu, H.; Yao, Y.; Chen, H.; Ren, C.; Wu, F.; Kannan, K. Occurrence and distribution of organophosphate flame retardants (OPFRs) in soil and outdoor settled dust from a multi-waste recycling area in China. Sci. Total Environ. 2018, 625, 1056–1064. [Google Scholar] [CrossRef]
- Xu, F.; Tay, J.H.; Covaci, A.; Padilla-Sánchez, J.A.; Papadopoulou, E.; Haug, L.S.; Neels, H.; Sellström, U.; de Wit, C.A. Assessment of dietary exposure to organohalogen contaminants, legacy and emerging flame retardants in a Norwegian cohort. Environ. Int. 2017, 102, 236–243. [Google Scholar] [CrossRef]
- Gilles, L.; Govarts, E.; Rambaud, L.; Vogel, N.; Castaño, A.; Esteban López, M.; Rodriguez Martin, L.; Koppen, G.; Remy, S.; Vrijheid, M.; et al. HBM4EU combines and harmonises human biomonitoring data across the EU, building on existing capacity-The HBM4EU survey. Int. J. Hyg. Environ. Health 2021, 237, 113809. [Google Scholar] [CrossRef]
- Miller, L.A.; Stapleton, F.B. Urinary volume in children with urolithiasis. J. Urol. 1989, 141, 918–920. [Google Scholar] [CrossRef]
- Lynn, R.K.; Wong, K.; Gravie-Gould, C.; Kennish, J.M. Disposition of the flame retardant, tris (1,3-dichloro-2-propyl) phosphate, in the rat. Drug Metab. Dispos. 1981, 9, 434–441. [Google Scholar]
- Wittassek, M.; Koch, H.M.; Angerer, J.; Brüning, T. Assessing exposure to phthalates-the human biomonitoring approach. Mol. Nutr. Food Res. 2011, 55, 7–31. [Google Scholar] [CrossRef]
- World Health Organization. Principles and Methods for the Risk Assessment of Chemicals in Food, International Programme on Chemical Safety, Environmental Health Criteria 240. Chapter 6: Dietary Exposure Assessment of Chemicals in Food. 2009. Available online: http://www.who.int/ipcs/food/principles/en/index1.html (accessed on 20 March 2022).
- European Food Safety Authority (EFSA). Comprehensive European Food Consumption Database. 2021. Available online: https://www.efsa.europa.eu/de/food-consumption/comprehensive-database (accessed on 25 April 2022).
- Stahl, A.; Vohmann, C.; Richter, A.; Heseker, H.; Mensink, G.B.M. Changes in food and nutrient intake of 6-to 17-year-old Germans between the 1980s and 2006. Public Health Nutr. 2009, 12, 1912–1923. [Google Scholar] [CrossRef]
- Elmadfa, I. Österreichischer Ernährungsbericht 2012. 2012. Available online: http://www.bmg.gv.at/cms/home/attachments/4/5/3/CH1048/CMS1348749794860/oeb12.pdf (accessed on 25 April 2022).
- De Ridder, K.; Bel, S.; Brocatus, L.; Cuypers, K.; Lebacq, T.; Moyersoen, I.; Ost, C.; Teppers, E. De consumptie van voedingsmiddelen en de inname van voedingsstoffen. In Voedselconsumptiepeiling 2014–2015. Rapport 4; Bel, S., Tafforeau, J., Eds.; WIV-ISP: Brussels, Belgium, 2016. [Google Scholar]
- Pedersen, A.; Fagt, S.; Groth, M.; Christensen, T.; Biltoft-Jensen, A.; Matthiessen, J.; Andersen, N.L.; Korup, K.; Hartkopp, H.; Ygil, K.; et al. Danskernes Kostvaner 2003–2008; DTU Fødevareinstituttet: Søborg, Denmark, 2009. [Google Scholar]
- ANSES. Third Study on the Food Consumption and Eating Habits of the French Population. 2017. Available online: https://www.anses.fr/en/content/inca-3-changes-consumption-habits-and-patterns-new-issues-areas-food-safety-and-nutrition (accessed on 20 March 2022).
- European Commission. European Union Risk Assessment Report Tris (2-chloro-1-methlyethyl) phosphate (TCPP); Chemicals Policy and Services Health and Safety Authority: Dublin, Ireland, 2008; Volume 57, pp. 98–419. [Google Scholar]
- Ali, N.; Dirtu, A.C.; Van den Eede, N.; Goosey, E.; Harrad, S.; Neels, H.; Coakley, J.; Douwes, J.; Covaci, A. Occurrence of alternative flame retardants in indoor dust from New Zealand: Indoor sources and human exposure assessment. Chemosphere 2012, 88, 1276–1282. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry. Toxicological Profile for Phosphate Ester Flame Retardants. Volume 153, pp. 451–459; 2012. Available online: https://www.atsdr.cdc.gov/toxprofiles/tp202.pdf (accessed on 20 March 2022).
- U.S Environmental Protection Agency’s (US-EPA). Provisional Peer-Reviewed Toxicity Values for Tris(2-chloroethyl)phosphate (TCEP) EPA/690/ R-09/069F; U.S Environmental Protection Agency’s (US-EPA): Cinicinnazi, OH, USA, 2009.
- WHO Environmental Health Criteria 209 Flame Retardants: Tris (chloropropyl) Phosphate and Tris (2-chloroetyhl) Phosphate. 2004. Available online: https://www.who.int/ipcs/publications/ehc/who_ehc_209.pdf (accessed on 20 March 2022).
- Vejdovszky, K.; Mihats, D.; Griesbacher, A.; Wolf, J.; Steinwider, J.; Lueckl, J.; Jank, B.; Kopacka, I.; Rauscher-Gabernig, E. Modified Reference Point Index (mRPI) and a decision tree for deriving uncertainty factors: A practical approach to cumulative risk assessment of food contaminant mixtures. Food Chem. Toxicol. 2019, 134, 110812. [Google Scholar] [CrossRef]
- Bastiaensen, M.; Gys, C.; Malarvannan, G.; Fotache, M.; Bombeke, J.; Ait Bamai, Y.; Araki, A.; Covaci, A. Short-term temporal variability of urinary biomarkers of organophosphate flame retardants and plasticizers. Environ. Int. 2021, 146, 106147. [Google Scholar] [CrossRef]
- Krystek, P.; Beeltje, H.; Noteboom, M.; van den Hoeven, E.M.; Houtzager, M.M.G. Analytical human biomonitoring method for the identification and quantification of the metabolite BDCPP originated from the organophosphate flame retardant TDCPP in urine. J. Pharm. Biomed. Anal. 2019, 170, 169–175. [Google Scholar] [CrossRef]
- Wang, X.; Zhu, Q.; Liao, C.; Jiang, G. Human internal exposure to organophosphate esters: A short review of urinary monitoring on the basis of biological metabolism research. J. Hazard. Mater. 2021, 418, 126279. [Google Scholar] [CrossRef]
- Xu, F.; Giovanoulis, G.; Van Waes, S.; Padilla-Sanchez, J.A.; Papadopoulou, E.; Magnér, J.; Haug, L.S.; Neels, H.; Covaci, A. Comprehensive study of human external exposure to organophosphate flame retardants via air, dust, and hand wipes: The importance of sampling and assessment strategy. Environ. Sci. Technol. 2016, 50, 7752–7760. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Acgencys (US-EPA). U.S EPA Update for of the Exposure Factors Handbook Chapter 5 (Update)-Soil and Dust Ingestion; EPA/600/R-17/384F; U.S EPA Office of Research and Development: Washington, DC, USA, 2017.
- Gbadamosi, M.R.; Abdallah, M.A.E.; Harrad, S. A critical review of human exposure to organophosphate esters with a focus on dietary intake. Sci. Total Environ. 2021, 771, 144752. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Food Category | TDCIPP | TCIPP | TCEP | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| df% | LB | MB | UB | df% | LB | MB | UB | df% | LB | MB | UB | |
| Animal and vegetable fats and oils and primary derivatives thereof | 0 | 5.7 * | 16.1 | 34.7 | 0 | 11 * | 31 | 66.8 | 11 | 1.55 * | 2.5 | 3.6 |
| Whole Eggs | 0 | 0 | 0.05 | 0.1 | 25 | 0.1 | 0.15 | 0.19 | 25 | 0.02 | 0.03 | 0.04 |
| Fish (meat) | 39 | 0.4 | 0.5 | 0.6 | 59 | 0.71 | 0.76 | 0.8 | 54 | 0.12 | 0.13 | 0.14 |
| Crustaceans | 0 | 0 | 0.22 | 0.44 | 20 | 0.18 | 0.22 | 0.26 | 0 | 0 | 0.04 | 0.07 |
| Grains and grain-based products | 0 | 0 | 0.16 | 0.31 | 71 | 3.58 | 3.65 | 3.73 | 57 | 0.6 | 0.61 | 0.63 |
| Meat and meat products | 0 | 0 | 0.8 | 1.61 | 26 | 0.19 | 0.29 | 0.39 | 34 | 0.15 | 0.2 | 0.25 |
| Milk | 0 | 0 | 0.21 | 0.43 | 0 | 0 | 0.8 | 1.59 | 0 | 0 | 0.23 | 0.45 |
| Cheese | 44 | 2.52 | 3.09 | 3.65 | 50 | 1.42 | 1.53 | 1.63 | 50 | 0.66 | 0.71 | 0.77 |
| Food Category | Consumption Data Germany 1 | Consumption Data Austria 2, * | Consumption Data Belgium 3 | Consumption Data Denmark 4 | Consumption Data France 5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total Mean Population | High Level Consumer Only | Total Mean Population | High Level Consumer Only | Total Mean Population | High Level Consumer Only | Total Mean Population | High Level Consumer Only | Total Mean Population | High Level Consumer Only | |
| Animal and vegetable fats and oils and primary derivatives thereof | 0.58 | 1.34 | 0.92 | 1.98 | 0.48 | 1.29 | 1.14 | 2.2 | 0.62 | 1.5 |
| Whole Eggs | 0.67 | 2.15 | 0.47 | 1.59 | 0.01 | 1.47 | 0.5 | 1.44 | 0.05 | 0.89 |
| Fish (meat) | 0.21 | 2.59 | 0.38 | 2.62 | 0.35 | 4.36 | 0.4 | 1.52 | 0.54 | 4.01 |
| Crustaceans | 0.0004 | 1 | 0.01 | 1.54 | 0.05 | 2.52 | 0.03 | 0.43 | 0.04 | 1.82 |
| Grains and grain-based products | 8.16 | 14.03 | 9.4 | 15.76 | 7.31 | 12.65 | 7.72 | 11.85 | 8.04 | 13.97 |
| Meat and meat products | 2.75 | 6.01 | 2.86 | 6.67 | 4.14 | 9.17 | 3.83 | 6.6 | 4.38 | 9.14 |
| Milk | 8.46 | 20.98 | 6.68 | 16.54 | 9.16 | 27.11 | 17.26 | 35.65 | 10 | 26.69 |
| Cheese | 0.74 | 2.28 | 0.89 | 2.25 | 1.09 | 4.37 | 0.73 | 1.88 | 2.05 | 6.07 |
| Country | OPFR-Metabolite | n | Df | Urinary Concentration [µg/L] | EDI of Parent Compound | ||
|---|---|---|---|---|---|---|---|
| [%] | [µg/kg bw/d] | ||||||
| Mean | High | Mean | High | ||||
| Belgium (3xG study) | BDCIPP | 133 | 98 | 1.03 | 3.08 | 0.05 | 0.14 |
| BCIPP | 133 | 13.5 | - | 1.4 | - | 0.063 | |
| Denmark (OCC study) | BDCIPP | 291 | 97 | 0.72 | 2.8 | 0.03 | 0.13 |
| BCIPP | 291 | 6.5 | - | 0.48 | 0.022 | ||
| France (Esteban study) | BDCIPP | 299 | 65 | 1.34 | 3.82 | 0.06 | 0.18 |
| BCIPP | 299 | 31 | - | 3.71 | 0.17 | ||
| Germany (GerES V study) | BDCIPP | 300 | 80 | 1.03 | 3.09 | 0.05 | 0.15 |
| BCIPP | 300 | 53 | 0.11 1 | 0.74 | 0.05 | 0.034 | |
| BCEP | 300 | 63 | 0.48 | 0.96 | 0.022 | 0.043 | |
| Slovenia (SLO CRP study) | BDCIPP | 147 | 84 | 0.86 | 2.32 | 0.04 | 0.11 |
| BCIPP | 147 | 18 | - | 0.6 | - | 0.027 | |
| BCEP | 147 | 20 | - | 4.79 | - | 0.214 | |
| Slovakia (PCB cohort study) | BDCIPP | 300 | 17 | - | 1.46 | - | 0.07 |
| BCIPP | 300 | 29 | - | 1.71 | - | 0.078 | |
| BCEP | 300 | 20 | - | 3.81 | - | 0.17 | |
| TDCIPP | TCIPP | TCEP | |||||
|---|---|---|---|---|---|---|---|
| MRL | RfD | RfD | MOS * | MRL | p-RfD | RfD | |
| (200 µg/kg bw/d) | (15 µg/kg bw/d) | (80 µg/kg bw/d) | (52 mg/kg bw/d) | (200 µg/kg bw/d) | (7 µg/kg bw/d) | (22 µg/kg bw/d) | |
| Belgium | 0.001 | 0.01 | 0.001 | 823,423 | - | - | - |
| Denmark | 0.001 | 0.01 | 0.0003 | 2,360,912 | - | - | - |
| France | 0.0009 | 0.01 | 0.002 | 307,619 | - | - | - |
| Germany | 0.0007 | 0.01 | 0.0004 | 1,538,093 | 0.0002 | 0.006 | 0.002 |
| Slovenia | 0.00054 | 0.0073 | 0.0003 | 1,908,470 | 0.001 | 0.03 | 0.01 |
| Slovakia | 0.0003 | 0.004 | 0.001 | 667,016 | 0.001 | 0.024 | 0.008 |
| Sources of Uncertainty | Direction |
|---|---|
| Dietary exposure estimates | |
| The use of aggregated occurrence and food consumption data | + |
| Occurrence data | |
| The used occurrence data were from a single study and from only one country | +/− |
| Concentration data are considered applicable for all items within the entire food category | + |
| Food consumption data | |
| The used food consumption data were at a low hierarchy level | + |
| The used food consumption data were collected between 2006–2014 and might be outdated | +/− |
| For Slovenia and Slovakia no food consumption data were available, data from the geographically closest region was used | +/− |
| Use of data from food consumption surveys of a few days to estimate long-term (chronic) exposure for high percentiles (95th percentiles) | + |
| Hazard data | |
| Ali et al., 2012 did not provide information on the toxicological study and endpoints from which the reference dose for TCIPP was derived | +/− |
| Health-Based Guidance Values are only based on limited toxicological data | +/− |
| Uncertainty factors ranged from 100 to 1000 | +/− |
| Estimated daily intake by using HBM data | |
| Extrapolation from single non-creatinine adjusted urine sample (spot or morning urine sample) to a 24 h urine sample | +/− |
| Slovakia and Denmark provided spot urine samples (less concentrated as first morning urine) | - |
| The estimated urinary molar excretion fraction (Fue) from TDCIPP was used for TCIPP and TCEP | +/− |
| Absence of individual urine excretion volume data | +/− |
| BCIPP was the only provided biomarker for TCIPP | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plichta, V.; Steinwider, J.; Vogel, N.; Weber, T.; Kolossa-Gehring, M.; Murínová, L.P.; Wimmerová, S.; Tratnik, J.S.; Horvat, M.; Koppen, G.; et al. Risk Assessment of Dietary Exposure to Organophosphorus Flame Retardants in Children by Using HBM-Data. Toxics 2022, 10, 234. https://doi.org/10.3390/toxics10050234
Plichta V, Steinwider J, Vogel N, Weber T, Kolossa-Gehring M, Murínová LP, Wimmerová S, Tratnik JS, Horvat M, Koppen G, et al. Risk Assessment of Dietary Exposure to Organophosphorus Flame Retardants in Children by Using HBM-Data. Toxics. 2022; 10(5):234. https://doi.org/10.3390/toxics10050234
Chicago/Turabian StylePlichta, Veronika, Johann Steinwider, Nina Vogel, Till Weber, Marike Kolossa-Gehring, Lubica Palkovičová Murínová, Soňa Wimmerová, Janja Snoj Tratnik, Milena Horvat, Gudrun Koppen, and et al. 2022. "Risk Assessment of Dietary Exposure to Organophosphorus Flame Retardants in Children by Using HBM-Data" Toxics 10, no. 5: 234. https://doi.org/10.3390/toxics10050234
APA StylePlichta, V., Steinwider, J., Vogel, N., Weber, T., Kolossa-Gehring, M., Murínová, L. P., Wimmerová, S., Tratnik, J. S., Horvat, M., Koppen, G., Govarts, E., Gilles, L., Rodriguez Martin, L., Schoeters, G., Covaci, A., Fillol, C., Rambaud, L., Jensen, T. K., & Rauscher-Gabernig, E. (2022). Risk Assessment of Dietary Exposure to Organophosphorus Flame Retardants in Children by Using HBM-Data. Toxics, 10(5), 234. https://doi.org/10.3390/toxics10050234